[ad_1]
Introduction
Sexual and reproductive health (SRH) is a key dimension of the health and wellbeing of individuals. Ideally, it should be addressed using a rights-based approach focusing on empowering people, especially young people, to make free and informed choices. Sexuality education (SE) is key to promoting the sexual wellbeing of young people and to preventing HIV and other sexually transmitted infections (STIs) (European Centre for Disease Prevention and Control Citation2013). The right to SE is embedded in the Universal Declaration of Human Rights (UN Citation1948) through the commitment to guarantee every human being protection for their health, wellbeing and dignity. The Programme of Action from the United Nations (UN) International Conference on Population and Development (Citation1994) explicitly urged governments to ensure the provision of school-based and community-based SE. This should be done so in a form that is age-appropriate, starts at an early age, promotes mature decision-making, is directed towards improving gender inequalities, and engages young people in planning, implementing and assessing activities.
It is widely recognised that school has an important role to play in learning about health. Although school-based SE (SBSE) alone may not be enough to ensure the rights of young people to SRH and prevent STIs, school programmes are a cost-effective way of contributing to these goals (Kivela, Ketting, and Baltussen Citation2013). The percentage of schools providing young people with life-skills-based HIV prevention and SE has become a key indicator in monitoring progress towards the attainment of international goals (UNESCO Citation2016a).
However, the nature of school-based SE varies considerably throughout the world. According to the 2016 Global Education Monitoring Report (UNESCO Citation2016a), basic school curricula and educational standards rarely include SE programmes. Multi-country reviews show limited progress in developing national policies and strategies for implementing SBSE or large-scale high-quality programmes (Haberland and Rogow Citation2015). Ketting and Ivanova (Citation2018) reported that out of the 25 European countries investigated, which did not include Italy, only 10 offered an approach to SBSE that could be considered “comprehensive’ as defined by the WHO Regional Office for Europe and BZgA (Citation2010). In 2020, 23 out of 49 European countries did not address sexual orientation and gender identity explicitly in school curricula (UNESCO Citation2020).
SE in general, and Comprehensive Sexuality Education (CSE) in particular, have a positive impact on young people, reducing i) the rates of in teenage pregnancy and abortion, ii) the incidence of STIs and HIV infection (Haldre, Part, and Ketting Citation2012; Apter, Dan Citation2011), sexual abuse (Bachus, Martens, and van der Sluis Citation2010) and homophobia (Bucx, Sman, and Jalvingh Citation2014). CSE seeks to empower vulnerable populations, such as young disabled people and/or LGBTQIA+ young people, to advocate for their rights and to recognise potentially abusive situations (McDaniels and Fleming Citation2016; Sondag, Johnson, and Parrish Citation2020).
CSE is an approach to SE that emerged in 2010. However, the meaning of the term ‘comprehensive’ was not well characterised and was used differently by a variety of authors and organisations (Frances, Miedema, and Le Mat Citation2018) until 2018, when UNESCO developed and promoted the now widely accepted definition:
“a curriculum-based process of teaching and learning about the cognitive, emotional, physical and social aspects of sexuality. It aims to equip children and young people with knowledge, skills, attitudes and values that will empower them to: realize their health, well-being and dignity; develop respectful social and sexual relationships; consider how their choices affect their own well-being and that of others; and, understand and ensure the protection of their rights throughout their lives” (UNESCO Citation2018, 16).
According to UNESCO, a comprehensive approach to SE focuses not only on the undesirable consequences of sexual activity, but also aims to promote the empowerment of young people throughout their lives, protecting their development, and providing the skills and information that will help them to understand and enjoy their sexuality within a framework of respect and consent towards themselves and others.
Despite several attempts to do so, the very first being the introduction of ‘sexual hygiene’ in schools back in 1902 (Rifelli and Ziglio Citation2006), Italy is one of the few European countries where SE is still not included in school curricula. It remains at the discretion of individual heads of school in Italy whether or not to endorse school policies promoting it (Cassar Citation2022). Italy still lacks a comprehensive policy/approach to SE that is consistently and equally implemented across the country.
The consequences of this gap in education include poor sexual health knowledge (Cegolon et al. Citation2020; Drago et al. Citation2016), low and inconsistent use of condoms and other forms of contraception (Panatto et al. Citation2012), limited access to services such as youth sexual health clinics (YSHCs) (Pizzi et al. Citation2020), high levels of gender-based violence (Italian National Institute of Statistics Citation2019) and homotransphobia (Osservatorio diritti Citation2019). Moreover, 20% of all STIs detected in Italy are among young people aged 15–24 (Salfa and Ferri Citation2021).
In recent studies, Italian students have identified schools as the most appropriate settings in which to provide young people with information about SE (Drago et al. Citation2016; Pizzi et al. Citation2020; Psaroudakis et al. Citation2020). In this study, therefore, we aimed to assess the current situation with respect to coverage, implementation and content of SBSE activities in middle and high schools in Italy between 2016 to 2020.
Methods
Desk review
Policy frameworks and educational projects on the prevention and control of STIs, carried out in secondary schools between 2016 and 2020, were identified for all 20 regions in Italy. The research was undertaken by consulting regional government websites, or Googling using specific keywords (STIs prevention, STIs regional resolution, youth educational project, and STIs in schools), and the name of each region. Additional documents (such as the National Plan on HIV/AIDS prevention) were shared directly by co-authors and their professional networks.
Survey
An online survey (SurveyMonkey©) was used to collect information from SBSE providers on the following: general information about the educational activity (EA) provider, geographical area covered, period of implementation of activities, length of the activities (e.g. hours spent with a class), type of schools targeted, personnel involved, goals/objectives and content covered, educational approach, educational tools used, products created by the students following the activity, and evaluation strategy. Respondents were invited to share the material used to implement the activities and/or any published reports.
The survey was disseminated at a national and regional level to relevant institutional bodies and civil-society organisations (CSOs). The following bodies or institutions were approached: CSOs listed by the Technical Health Committee for HIV/AIDS of the Italian Ministry of Health; other local or national organisations known to be providing SE in schools; local health authorities across the country; professional associations of sexologists; and independent SE educators. The survey was sent to approximately 850 recipients in total (). To widen dissemination and maximise the likelihood of getting a reasonably representative sample across different sub-national areas, a regional contact point was established in four regions in the country – Lombardy, Tuscany, Lazio and Apulia – along with a web mailbox dedicated to the project. The mailbox was used to distribute survey invitation letters, provide feedback and online support to respondents, and to collect the materials.
Table 1. Number of contact emails sent per type of provider.
Survey analysis
A descriptive analysis was conducted using data obtained from the online survey and facilitated by the use of IBM SPSS Statistics 26. A qualitative analysis was conducted to further assess the nature of the EAs reported in the survey. We adapted the UNESCO (Citation2016a) to develop a qualitative analysis framework focusing on three domains: programme, implementation and results.1 Each domain included three or four sub-categories. The framework we used was piloted with a subset of 25 EAs.
The operational definition of SE employed by the study was: an EA delivered over at least two sessions (≥4 hours), covering ‘affectivity and sexuality’ and three other topics from those listed in the survey. Information was extracted concerning the goals, methods and materials. EAs that did not meet these criteria were classified according to their main objective into one of the following additional categories:
-
STI prevention: any EA describing STIs, symptoms and complications; STI prevention; healthcare services for STI diagnosis, treatment and care
-
diversity education: any EA focusing on social stigma and discrimination, bullying, gender-based violence and homo-bi-transphobia
-
healthy lifestyle education: any EA focusing on the promotion of healthy and safe lifestyles, online risks connected to sexuality, and risk-avoidance related topics (e.g. substance abuse)
Findings
Desk review
A total of 34 policy frameworks published between 2016–2020 were identified on the web. These mostly took the form of resolutions (n = 22), prevention plans (n = 11) and other documents (n = 1). The geographical distribution of these documents was uneven, with the majority (53.0%) relating to regions in the north of Italy. No documents were found for two regions (Marche and Sicily). Among the regions with at least one document available (n = 18), one region (Veneto) had four documents associated with it, and the remainder had between one and three.
Thirty-two documents reporting on EAs for middle and high school children were identified by the web-based research. All of these were aimed at STI prevention and used methods such as peer-education, group activities, and formal didactic lessons using both paper and digital materials. A total of 62.5% of the EAs were carried out in regions in the north. In eight regions (Valle d’Aosta, Umbria, Abruzzo, Basilicata, Calabria, Apulia, Sicily and Sardinia), no documents describing EAs were found. In one region (Piemonte) six EAs were identified, while for the remaining eleven regions, between one and five EAs were identified. None of the documents retrieved included reports on any evaluation activities.
Survey
A total of 232 SBSE activities were reported in the surveys to have been carried out during the study period. Of these, 219 took place in secondary schools, and 13 in primary schools. Data from the primary schools were not analysed further since this was not within the scope of the present study. Most interventions (65.0%) were conducted by CSOs. The reported objectives included: information provision (37.4%), awareness raising (26.8%), and student education (e.g. peer education) (8.2%) (Figure 1).
All authors
 , Ludovica Colaprico, Massimo Oldrini, Marco Ubbiali, Anna Caraglia, Domenico Martinelli , Luigina Mortari, Anna Teresa Palamara, Barbara Suligoi & Lara Tavoschi
, Ludovica Colaprico, Massimo Oldrini, Marco Ubbiali, Anna Caraglia, Domenico Martinelli , Luigina Mortari, Anna Teresa Palamara, Barbara Suligoi & Lara Tavoschi Figure 1. Objectives of the educational activities.
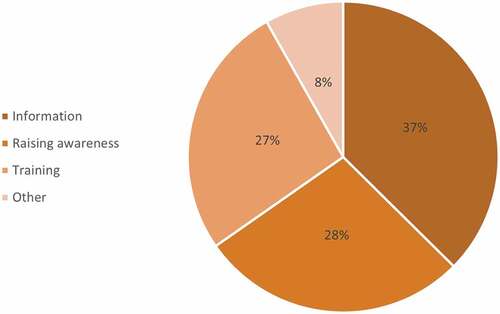
Figure 1. Objectives of the educational activities.
Analysis of the geographical distribution of the SBSE activities showed that 94 (42.9%) activities had been conducted in central Italy, 87 (39.7%) in the north, and 38 (17.4%) in the south. The activities mostly took place in the four target regions: Lazio (48–21.9%), Lombardy (47–21.5%), Tuscany (41–18.7%), and Apulia (15–6.8%). In addition, 11 SBSE activities had been conducted in Emilia-Romagna (5.0%), 10 in Veneto (4.6%), and 47 (21.5%) in the remaining regions. The activities identified took place in 5,879 secondary schools between 2016 to 2020 (Figure 2).
All authors
, Ludovica Colaprico, Massimo Oldrini, Marco Ubbiali, Anna Caraglia, Domenico Martinelli , Luigina Mortari, Anna Teresa Palamara, Barbara Suligoi & Lara Tavoschi Figure 2. Number of secondary school students reported to be involved in the educational activities (2016–2020).
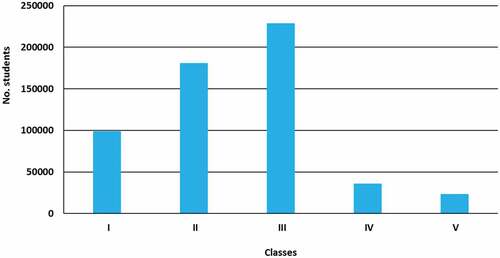
Figure 2. Number of secondary school students reported to be involved in the educational activities (2016–2020).
The main topics covered were: promotion of safe behaviours/lifestyles, STI prevention, relationships and sexuality. The main tools used to carry out SBSE activities were: active learning methods (150–68.5%), multimedia material (144–65.8%), printed material (122–55.7%), and videos (119–54.3%). The most frequently used methodologies were active learning (151–68.9%), formal didactic lessons (131–59.8%) and peer education (55–25.1%). No specific outputs were associated with 67 (30.6%) SBSE activities. In the remaining 152 (69.1%) activities, outputs from students included: scheduled peer education meetings (63–28.8%), paper materials (documents, booklets, flyers, brochures) (62–28.3%), digital and multimedia materials (50–22.8%), events (theatrical performances, exhibitions, stands and info points) (38–17.4%), and gadgets (16–7.3%). Factors rated the most positively in relation to the activities in schools were the active participation of students and the presentation of content in a straightforward, simple language. The most criticised issue was the limited time allocated to SBSE activities within the school. In more than half of the activities (111–50.7%), evaluation was carried out by means of satisfaction and/or learning assessments. The results from these are available from the corresponding author upon request.
The qualitative analysis involved 216/219 SBSE activities, due to insufficient information for three of them. Of these, 62 (28.7%) were classified as CSE activities, of which 30/62 (48.4%) had been developed and provided by local health departments or youth sexual health clinics, 31 (50%) by CSOs, and 1 (1.6%) by independent educators (Figure 3). The non-CSE activities (154/216-71.3%) were classified in terms of their main objectives and reported content: 75 (48.7%) focused on STI prevention, 31 (20.1%) addressed healthy lifestyles, and 21 (13.6%) took the form of diversity education (13.6%). The remaining 27 SBSE activities were categorised as ‘other types of activity’ (17.5%) or ‘unclassifiable’, as the information provided did not meet the analysis criteria (Figure 4).
All authors
, Ludovica Colaprico, Massimo Oldrini, Marco Ubbiali, Anna Caraglia, Domenico Martinelli , Luigina Mortari, Anna Teresa Palamara, Barbara Suligoi & Lara Tavoschi Figure 3. Educational activities classified as CSE or non-CSE, by type of provider.
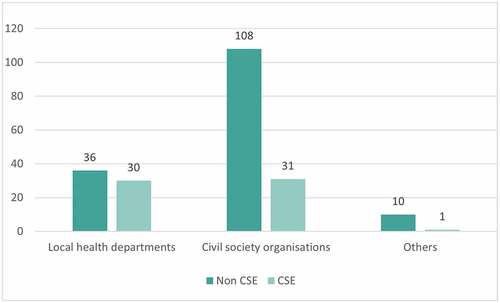
Figure 3. Educational activities classified as CSE or non-CSE, by type of provider.
All authors
, Ludovica Colaprico, Massimo Oldrini, Marco Ubbiali, Anna Caraglia, Domenico Martinelli , Luigina Mortari, Anna Teresa Palamara, Barbara Suligoi & Lara Tavoschi Figure 4. Classification of educational activities reported.
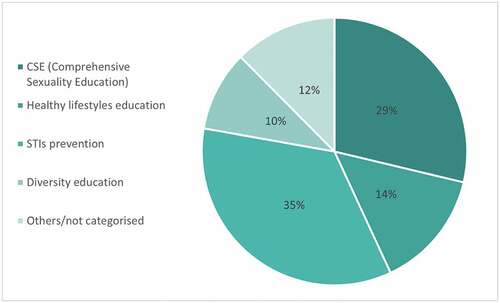
Figure 4. Classification of educational activities reported.
The median duration of the CSE activities was three sessions lasting a total of six hours, in contrast to the reported median of one session and four hours for non-CSE activities. Many non-CSE activities took the form of single session interventions (66/154-42,9%). Concerning the methodology, 34/62 CSE activities (54.9%) took the form of mixed method interventions (e.g. formal didactic lessons and group activities), with only 3/62 activities (4.8%) consisted of formal didactic lessons alone. The percentage of mixed method sessions was slightly lower for non-CSE activities (48%). A total of 20/154 (13%) of non-CSE activities consisted mainly of formal didactic lessons; however, the majority also included activity-based interventions with students. In 51/62 (82.3%) of CSE activities, school teachers were involved in the planning or provision of the activity, in 22/62 (35.5%) parents were involved, and in 20/62 (32.3%) other professionals participated (e.g. physicians, psychologists). In non-CSE activities, teachers were involved in the planning or provision of the activity in 109/154 cases (70.8%), with parents being involved in 35/154 cases (22.7%). Other professionals were involved in 60/154 activities (39%).
Student satisfaction was assessed in 40/62 CSE activities (64.5%) and in 77/154 of non-CSE activities (50%). An evaluation was conducted in 37/62 CSE activities (59.7%) based on knowledge and satisfaction, while a post-assessment survey took place in 31/62 (50%) cases. Both pre- and post-assessment surveys were distributed among participants in 26/62 (41.9%) CSE activities. According to the available data, all of the SBSE activities (26/26) were associated with an increase in knowledge and skills, while 15/26 (57.7%) also triggered some form of behaviour change. Of the non-CSE activities, 50/51 (98%) were associated with an increase in knowledge and skills, while 27/51 (52.9%) reported a change in behaviour. summarises these findings.
Table 2. Objectives of educational activities, implementation and results: CSE versus Non CSE.
Discussion
This study is the first attempt to provide an overview of the current situation with regards to SBSE activities in secondary schools in Italy. The findings reveal a highly heterogeneous picture, with much variation in terms of objectives, content and methods used to address SE-related topics. This variation is not surprising given the absence of a national standard for SE in school settings.
A number of different providers were shown to be involved. CSOs were responsible for 142/219 (64.8%) of the reported SBSE activities in the study. However, CSOs are a highly diverse group of entities and differ in terms of their values, objectives and desired outcomes (e.g. family planning, STI prevention, challenging homo-trans-negativity). The lack of national standards may also help to explain the inconsistent coverage of activities across the country. Metropolitan cities and central and northern regions appeared to be the best served areas, leaving behind the vulnerable young people in the more deprived southern regions.
Both during and after this study, the COVID-19 pandemic impacted the delivery of SBSE. While the number of schools involved in SE-related activities increased between 2016 and 2020, these activities were ground to a halt by the pandemic (Figure 5). The partial restart of face-to-face teaching in the 2020–21 school year did not result in a relaunch of activities, since the time available was limited. As highlighted in our findings, the limited slots given over to SE in the school timetables meant that many activities are carried out as single session interventions, raising questions about their educational value and capacity to promote change. The problem is that SE is not a formal part of the school curricula in Italy.
All authors
, Ludovica Colaprico, Massimo Oldrini, Marco Ubbiali, Anna Caraglia, Domenico Martinelli , Luigina Mortari, Anna Teresa Palamara, Barbara Suligoi & Lara Tavoschi Figure 5. Number of schools that had undertaken educational activities per school year.

Figure 5. Number of schools that had undertaken educational activities per school year.
Without statutory inclusion, there will always be a barrier to the allocation of adequate time and resources. Nearly all the students aged between 16–17 who were interviewed in the most recent Studio Nazionale Fertilità (National Fertility Study) undertaken for the Italian Ministry of Health) stated that schools should undertake sexuality and SRH education (Pizzi et al. Citation2020), confirming previous findings from 2000. Moreover, 63% of these students suggested that instead of regular teachers, external educators should be involved in providing SBSE. The report also highlighted how young people tend to overestimate their knowledge of sexuality and SRH, and revealed how widespread erroneous beliefs regarding sexuality are.
Italian students score poorly in terms of sexual health knowledge and awareness in a variety of studies. For example, in recent studies the majority of young people did not have accurate knowledge of how birth control works (Cegolon et al. Citation2020), which infections can be transmitted sexually (Drago et al. Citation2016), or what a sexual health clinic for young people is and how to access one (Pizzi et al. Citation2020). Moreover, only a small percentage of the young people interviewed mentioned having received SE in school.
When it was provided, the SBSE focused mainly on risk prevention, and sexual health topics such as STI prevention and contraception. In contrast, sexuality education guidelines developed by international institutions such as UNESCO (Citation2018), the WHO Regional Office for Europe and BZgA (Citation2010) and the International Planned Parenthood Federation (IPPF) (Citation2017) report that good quality SE should address not only sexual health topics, but also human rights, gender-based violence, sexual identity and active citizenship. This education activity should, moreover, promote a positive and inclusive view of sexuality as a key part of human life. Sexual wellbeing has been defined in terms of the seven different domains of sexual safety and security, sexual respect, sexual self-esteem, resilience in relation to sexual experiences, forgiveness of past sexual experiences, sexual self-determination, and comfort with sexuality. This means that SBSE should be a core subject focused on promoting the sexual wellbeing of young people as part of a comprehensive approach to sexuality (Mitchell et al. Citation2021).
Our results show that evaluation of SBSE activities in Italian schools rarely takes place and, if it occurs, findings are poorly documented. Evidence-based evaluations are essential for assessing not only the outcomes but also the planning, provision and reception of an intervention (Ketting, Friele, and Michielsen Citation2015; UNESCO Citation2016b). Examples of possible outcomes include adverse health-related outcomes such as new STIs and unwanted pregnancies; individual wellbeing outcomes such as positive mental health and a satisfying sex life; and social fairness outcomes related to levels of gender, and sex related discrimination. The continuing lack of well-documented evaluations of SBSE programmes and activities in Italy masks the benefits of the interventions. This in turn feeds perceptions of need on the part of policy makers and governments.
Limitations
This study had some limitations. First, the survey was distributed during the COVID-19 pandemic, when most SBSE activities were interrupted, and providers were focused on pandemic related issues. Additionally, not all the pertinent documents may have been retrieved due to the limited digitalisation of documents in Italy. This may also have contributed to the unequal geographical distribution of the documents identified. Although the survey was disseminated widely across the country, the number of respondents (particularly from certain regions) was limited. This may have resulted in a lack of completeness and representativeness of the findings. Finally, our operationalisation of CSE and non-CSE activities was pragmatic and was based on the responses to the survey questions, which aimed to collect information on many but not all the aspects of CSE. Our qualitative analysis of the findings may also have been affected by the possible inaccuracy and incompleteness of the information provided by the respondents.
Conclusions
Although many attempts have been made to introduce SE into the school curriculum, SE remains a controversial subject in Italy. This is largely due to societal, cultural, religious and political factors (e.g. myths about SE promoting early or promiscuous sexual behaviour, political opposition to the inclusion of LGBTQIA+-related topics, or the belief that SBSE denies parents the right to educate their children in accordance with their own values. As a result, young people suffer. A comprehensive approach towards SBSE, in line with international guidelines is thus strongly needed, as supported by multi-country evidence, and called for by the young people themselves.
To tackle this issue, national government and institutions, especially schools and educational agencies, should advocate for the integration of SE within the school curriculum and promote its implementation. Ideally, SBSE should be introduced into curricula as a cross-curricular theme, or included as a topic addressed in other disciplines, such as citizenship education, with which it shares some objectives and content. If introduced as a cross-curricular theme, the completeness and accuracy of SBSE should be supported through the appointment of a curriculum lead, and implemented by the teachers of different subjects specially trained and supported by external experts from a variety of disciplines (e.g. psychologists and sexologists, andrologists, gynaecologists and obstetricians, as well as health and education professionals).
Appropriate time should be allocated to the introduction of SBSE within the school timetable and supported by the active involvement of local health services such as youth sexual health clinics, appropriate disease prevention and vaccination departments, and relevant CSOs. In order to ensure as wide an impact as possible, a wide range of stakeholders should be involved, including parents, non-teaching school personnel, and community leaders. Activities should be tailored to students’ special needs and promote inclusivity, taking into account individual, cultural and religious sensitivities. Lastly, sexual health promotion and wellbeing skills should be integrated into the curricula of universities and colleges, with multidisciplinary training for health and education professionals.
[ad_2]
Source link